
Caritas India in partnership with the National Vector Borne Disease Control Programme (NVBDCP) under the Intensified Malaria Control Project-3 has been intensifying the elimination of Malaria from India, particularly in North East India. In Manipur under the Diocesan Social Service Society Imphal, Caritas India has walked the nooks and corners of the state to make people aware prevent and treat from the dreadful Malaria endemic. The given below details are of the present status of DSSS, the IMCP3 project.
Goal:
To reduce malaria related mortality by at least 50% and morbidity by at least 50% in project areas (08 states) by 2017 as compared to 2012.
Objectives:
- To achieve near universal coverage (80%) by 2017 by effective preventive intervention (LLIN) for population living in high risk project areas (API>1).
- To achieve near universal coverage (80%) of fever cases by correct, affordable and appropriate parasitological diagnosis; and prompt, effective treatment according to the national drug policy in project areas by 2017.
- To achieve 100% coverage in project areas by appropriate BCC activities to improve knowledge, awareness and responsive behaviour regarding effective preventive and curative malaria control interventions by 2017.
- To strengthen surveillance and M&E, program planning and management, and coordination and partnership development to improve service delivery in project areas by 2017.
- To strengthen health systems, community systems through capacity building (training) to improve service delivery in project areas by 2017.
Impact Indicators
- Confirmed malaria cases (microscopy or RDT) per 1000 persons per year
- Number of confirmed malaria deaths
- Total Positivity Rate (Microscopy + RDT)
| EPIDEMIOLOGICAL STATUS 2015 | ||||||
|---|---|---|---|---|---|---|
| Population | ABER | API | TPR | SFR | Death | |
| District (Chandel) | 46,325 | 0.01 | 0 | 0 | 0 | Nil |
| District (Churachandpur) | 1,35,676 | 6.78 | 0.01 | 0.02 | 0.01 | Nil |
| District (Tamenglong) | 1,01,037 | 0 | 0 | 0 | 0 | Nil |
| Total for DSSS coverage areas | 2,83,038 | 6.79 | 0.01 | 0.02 | 0.01 | Nil |
| Population | MBER | TPR | TFR | Death | |
| JAN 2016 | 2,83,038 | 0 | 0 | 0 | 0 |
| FEB 2016 | 2,83,038 | 0 | 0 | 0 | 0 |
| MARCH 2016 | 2,83,038 | 0 | 0 | 0 | 0 |
| APRIL 2016 | 2,83,038 | 0 | 0 | 0 | 0 |
| MAY 2016 | 2,83,038 | 0 | 0 | 0 | 0 |
| JUNE 2016 | 2,83,038 | 1.0 | 1.35 | 1.35 | 0 |
| JULY 2016 | 2,83,038 | 0.0 | 0 | 0 | 0 |
| August 2016 | 0.48 | 0.42 | 0.21 |
In the year Oct 2015 – Sept. 2016 the following activities were carried out by DSSS under IMCP3 project in Manipur:
DISTRIBUTION OF LONG LASTING INSECTICIDAL NETS (LLIN)
The distribution of LLINs in the high risk project areas had become imperative based on the project goal to ‘reduce malaria related mortality by at least 50 % and morbidity by at least 50% in project areas (08 States) by 2017 as compared to 2012’ and the project objective no. 1 which states the need to achieve near universal coverage (80%) by 2017 by effective preventive intervention (LLIN) for population living in high risk project areas (API>1)
| Sl. No | Name of the District | No. of LLINs distributed | No. of Villages reached |
|---|---|---|---|
| 1 | Churachandpur | 5342 LLINs | 58 villages |
| 2 | Chandel | 1524 LLINs | 22 villages |
| 3 | Tamenglong | 2273 LLINs | 12 villages |
Important of LLIN distribution is to -

Activity 1: Workshop on identifying concrete measures to control and prevent HIV/AIDs and drug
abuse and framing acceptable norms for the village development committee leaders
The program was designed to align responsibilities of the village level leaders in prevention of HIV transmission and drug abuse in their respective areas. Two programs were conducted in each of the districts. Group exercises were carried out to identify the problems and introduce concrete measures to control and prevent on HIV/AIDS transmission and drug abuse. Thus, the village level leaders draft an acceptable norms, facilitated by the chiefs/chairman and SAGs leaders with the assistance of the project staffs.
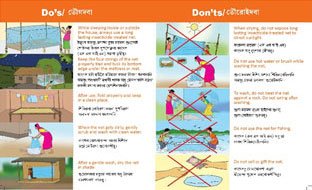
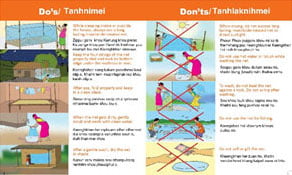
DOS & DON’T’S OF LLIN USAGE
Behavioural Change Communications (BCC)
The behaviour change communication (BCC) is an activities which are utilised to create awareness and prevention about Malaria in communities, villages, schools etc. The main components of BCC activities are:
- Infotainment- creating Malaria awareness through information with entertainment through the means of Audio- Visual devices.
- Miking- It is a public announcement about Malaria awareness in remote villages
- Community Consultation & Message Dissemination Activity (CCMD) – it is done with the village’s elders, women society and youth clubs in the villages to create platform to discuss about Malaria in the village for prevention.
Local School Activity
To educate the young minds of school students about Malaria the Local School Activity (LSA) was started to among the local schools. The aim of the LSA is to:
- to make students the leaders in putting into action malaria prevention activities in their school and village
- to make them resolve to strive to protect their school, family and community and themselves from Malaria by spreading AWARENESS AND PROMOTING GOOD BEHAVIORAL PRACTICES to fight the disease.
- To be a ROLE MODEL to their fellow students
The main activity of the program was:
- Extempore speech on Malaria
- Drawing competition on Mosquito bite
- Debates/Quiz on Malaria etc.
WORLD MALARIA DAY
Diocesan Social Service Society (DSSS) Imphal District Project Management Unit – Chandel INTENSIFIED MALARIA CONTROL PROJECT
Objectives:
- Creating mass awareness on malaria in the district and villages.
- Making people responsible for the control and prevention of Malaria in towns and villages
- Multi-sectorial involvement in the fight against malaria.
Events:
- Organizing mass rally at Chandel Town.
- Display of banners and hoardings in public places.
Participants:
- School children
- Govt. Officials
- IMCP-3 staffs
Outcome:
- More people become aware about the causes and prevention of malaria among the school going children.
- More people will come to understand the burden of Malaria diseases in their socio – economic status.
- People availing the health care facilities from the CHVs in their respective villages.
- More and more people getting involve in the control and prevention programs of malaria.
World Malaria Day Program
The World Malaria Day 2016 under the the “End Malaria for Good” was observed at Chandel headquarter organised by the District Management Unit – Chandel of Diocesan Social Service Society (DSSS) Imphal on 25th April 2016. The main objective of the event was to spread mass awareness on Malaria. President of All Tribal Women Organisation Chandel, Lalam Maite attended as chief guest. She was also accompanied by her friend Athong Haokip, Joint secretary of ATWO, Chandel. More than 300 students from several schools including St. Peter Hr. Sec. School, Emmanuel High School, TMT High School and Oriental High School took part in the event. Mr. Kh. Simon, DPO welcome everyone for the programme. He also highlighted the programes of IMCP – 3 and its goals and objectives Speaking on the occasion, ATWO president Lalam Mate asserted that proper awareness with effective mechanism to prevent and control malaria should be given to people living in different places of the state by concerned department with the help of NGO and other CBOs. Inspector Gaithoipou – OC Chandel P.S also spoke on the occasion and urged the students to be an active agent to end malaria in Manipur.
Mass Rally
A rally was flag off by District Malaria Officer, Chandel Dr. Joyson Mathew Monsang in the presence of the rallies and other dignitaries. It started from Indoor stadium and proceeded to DC junction. Each students were given flag card which different wordings on malaria. The tableau was beautifully decorated and mike announcement was carried out the rally. The security measures were given till the end of the rally. The rallies holding the flag card walked in two rows. The messages were loud and clear that malaria is diseases that can be eradicated in the districts, states and nation by collective efforts. Urging everyone to join fight against malaria the rallies displayed their oneness and importance of spreading the awareness on malaria by walking a long distance in the hot sun.
COMMUNITY HEALTH VOLUNTEERS TRAINING (CHVs)
The Community Health Volunteers are the most important persons of the IMCP3 Project. They under the supervision of the field Supervision implements the project at the village level. They perform Malaria Fever tests (RDT/Slides) and conducts BCC activities. Therefore their training is must for the project to be successful. Under DSSS we have 871 CHVs. By Sept. 2016 all the CHVs were trained under the proper guidelines to implement the IMCP3 project in hard reach remote area of Manipur.
Objectives of CHVs training:
- CHVs are trained on prevention, diagnosis and treatment of malaria as per national guidelines
- CHVs are trained on Behaviour Change Communication, community mobilization activities
- CHVs are trained on recording and reporting
- CHVs are trained on coordination at village level
ONE DAY CHV TRAINING PROGRAMME
Conducted by DPMU Tamenglong under Diocesan Social Service Society Imphal
Caritas India Consortium, IMCP3
Venue: Community Hall, Kekru Naga village.
Date: 21st September 2016.
Batch No: 03
No. Of CHV present: 23 CHVs.
The one day CHV training for the Community Health Volunteers of Longpi cluster and Gallon cluster under Nungba CHC was conducted at the Community Hall of Kekru Naga village on the 21st of September 2016. There were 23 CHVs who attended the training programe. The training started with the registration of the CHVs followed by a short invocation by the V/A member. Pre-test session followed by a brief introduction and words of welcome was given by the DPO. The training was facilitated by the DPMU staff along with the support of the Field Supervisors of the two cluster – Mr. Guigailung and Mr. Thankson Kameih. Mr. Philip Rongmei consultant of DVBDCP Tamenglong district took the technical session on malaria, its causes, its signs and symptoms, modes of transmission. He also described in brief the life cycle of the malaria parasites, the various prevention measures that needs to be put into practice by the community members. He also explained in detail the diagnosis, and treatment of malaria cases with practical demonstration on how to do the RDT test and prepare the Blood slides.
The DPO Mr. Jacob Pamie took a session on how to manage and record the stocks received from the DPMU office including filling of the various reporting forms – M1, M2, BCC input forms. He explained in detail the various BCC activities that are to be conducted by the CHV in the village for purposes of giving information, increasing the awareness and knowledge level of the Community members about malaria like miking, infotainment, community consultation and message dissemination and local school activity along with the incentive amount for each of the activity including the RDT test and the complete treatment incentive. He also stressed on the need for proper filling of the CHV diary wherein every CHVs are required to fill in the details of stocks received from the DPMU during the month and prepare the stock reconciliation in the M1 form. He requested the CHVs present to fill the various forms properly with all the supporting documents for the expenditures like getting pucca bills, and receipts without which their reports will be rejected and the expenditures incurred will be disallowed resulting in recovering the same from them.
The DPO also explained in details the levels of reporting under IMCP-3 project and the importance of reporting on time. He insisted that whatever activities conducted by the CHVs in the village with regards to IMCP-3 should be recorded in their diary and reported to the DPMU. The DPO also explained that the all the CHVs under each Field supervisors are required to come together for a day for discussion, planning and learning session every quarter according to their convenient time and place for which the project will provide the chv a flat rate of Rs. 310/- as TA/DA which will be paid through their respective bank account. The DPO pointed the need and the importance of opening bank account by all the CHVs for such incentive payment. He strictly instructed the CHVs that in future no incentive will be paid in cash and those CHVs who doesn’t have the bank account will not receive their incentives. With the post test the one day training program of the CHV came to an end at 4:00 pm.
EMERGENCY RESPONSE TO FEVER OUTBREAK AT LUNGCHIN VILLAGE
Our intervention
According to Census 2011 information the location code or village code of Lungchin village is 269854. Lungchin village is located in Singngat Tehsil of Churachandpur district in Manipur, India. It is situated 80km away from district headquarter Singngat. Singngat (32 km from Churachandpur) is the sub-district headquarter of Lungchin village. Lungchin has a total population of 633 peoples. There are about 103 houses in Lungchin village .
On the 14th July, 2016. : Mr. M. Khamkholian, & Mr. Goulunlal Naulak, two Field supervisors at the request of the DPO have started for the MISSION for Lungchin cluster by bike early morning and headed for Lungchin village directly. They were stopped by the Army at different check post situated along the Tedim Road and Guite Road. The road was filled with mud and water clogs like swimming pools. In most of the places, they have to push the bike, clean the mud which filled the space between the tyre and the mudguard.

They reached Suangdoh village by 1:00 pm. The army posted here promised to extend their help, if needed. Travelling through the not-frequently travelled inter-village road was tiring, but the urgency of the situation gives them more enthusiasm to save lives. The numerous falls they had on the way made them understand their situation more and more.
With no time to waste in reporting their presence to the village chief, they started entering each house, starting from the first house on their way, performing malaria test with the RDT kits and taking blood slides they have with them. They started with the one who are more serious. As informed most of the households in the village has ½ sick persons. Some were recovering and some are still in critical condition, unable to eat or drink due to their sickness. All the sick persons were reported to have high fever with chills, headache, nausea and general body weakness. The signs and symptoms were similar to malaria.
The only treatment most of them have taken is 1 or 2 tabs of Paracetamol (mg not recorded). “My thoughts linger on with one patient in the village, which I would like to share with you all here” said Mr. M. Khamkholian, “The patient is a boy of 9 years old. He lives with his parents and a younger sister about 6/7 years. He has been bed ridden for 2 days without taking food or medicine. His parents are in their jhum cultivation field as it is the high time for clearing the weeds. I look at the patient, the condition of the house they called their home. Instead of empathizing with the patient, my sympathy for him and his younger sister who sits by his side filled me with sympathy. I gave him all the biscuits I have with me and 5 tabs of paracetamol to sooth his high temperature.

As expected one test is positive for malaria. Medical Officer in-charge of Singngat PHC and his team have been there since morning. We come to know of it only when we met in the village chief’s residence. We gathered whoever is present in the village and talked to them about the need for correct and consistent use of LLIN provided by the government or any other mosquito net available, different methods of prevention (from mosquitoes and malaria) like cleaning of the surrounding, covering of water tanks etc. The chief, his Village Authority members and whoever is present on that day were happy to see a representative from an organization other than the government. Dr. Jamthianlal Valte also expressed his appreciation as we brought with us the RDK test through which we confirmed the sickness is not malaria. As the night is approaching, they wanted us to stay but we have another village to visit, as per the instruction of the DPO”. Ngaljang is another village is not so far from Lungchin, but due to the bad condition of the road, they managed to reach there by 7:00 PM. Many of the villagers have slept. They enquired about the sick persons, perform malaria test with RDT and take blood slides. They found no malaria here too.
A small intervention though but this trip has given us a lot in terms of emergency preparedness, how to deal with people and control my emotion as a service provider. The people trust our esteemed organization DIOCESAN SOCIAL SERVICE SOCIETY (DSSS) and CARITAS INDIA more than they have in the past. We believe, this small intervention will linger on in their mind if the same or similar situation arises again. The information we have given to them about malaria, its prevention and diagnosis will be more effective than the previous talks we have organized in the area.We are glad that DSSS/Caritas India through the IMCP3 project gave a platform to work with joy to serve our own people with proper system and medical preparedness in times of health emergency and need.